Video
Below is a quick video snap shot of this article.
Definition
When there is a progressively prolonged PR interval that eventually leads to a failed conduction through the AV node.
Another way of thinking of this is there is a progressively prolonged delay in the AV node until there is an instance where the impulse does not pass through the AV node.
A common way to remember this is “longer longer drop, then you got a Wenckebach.”
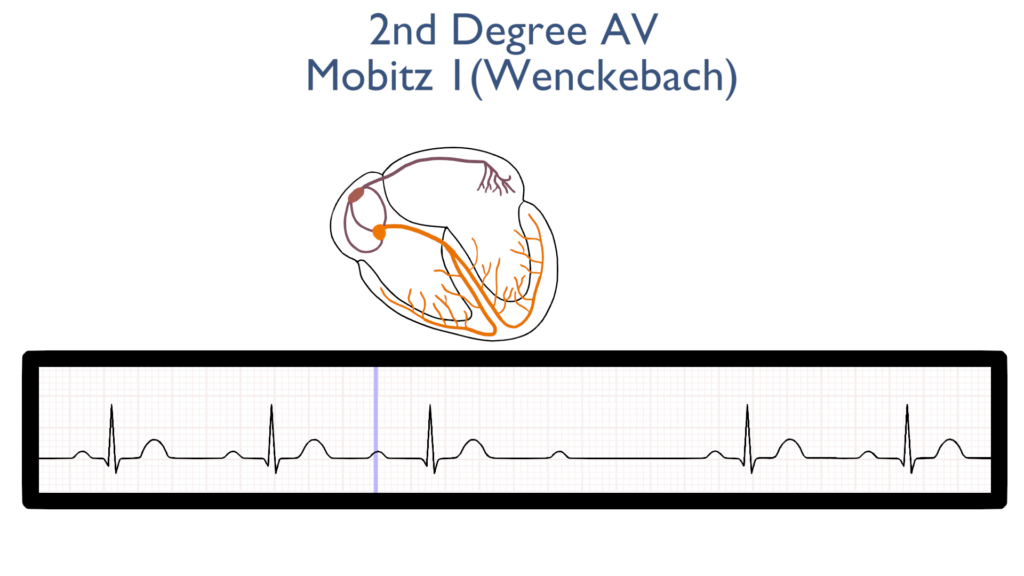
What’s happening in the heart
Atrial Contraction
First, the impulse originates in the SA node just as it does with a normal sinus rhythm.
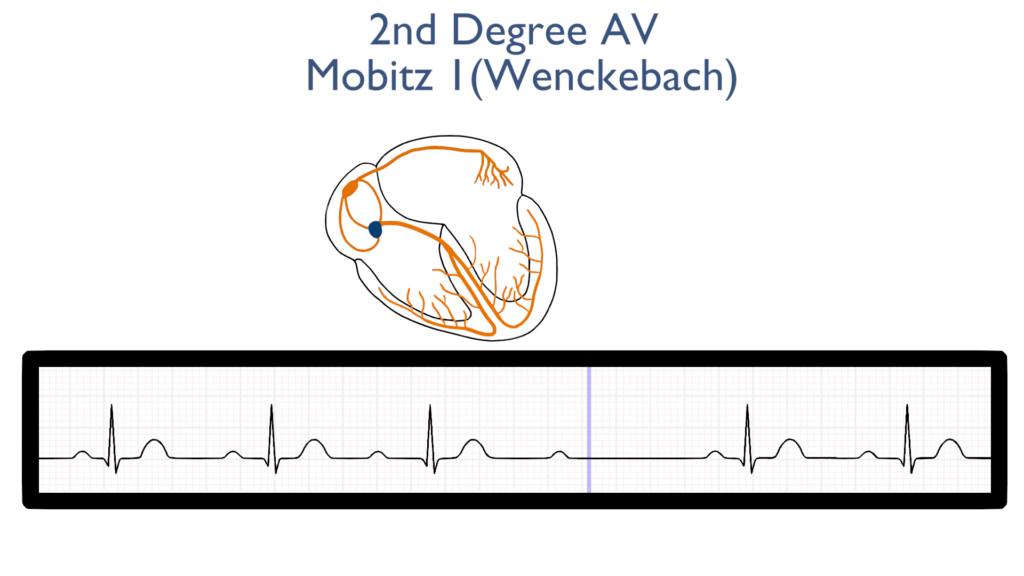
AV Node Delay
Next, there is a delay in the AV node just as there is with a normal sinus rhythm but with each beat this delay becomes progressively longer until it fails to conduct through the AV node to the bundle branches.
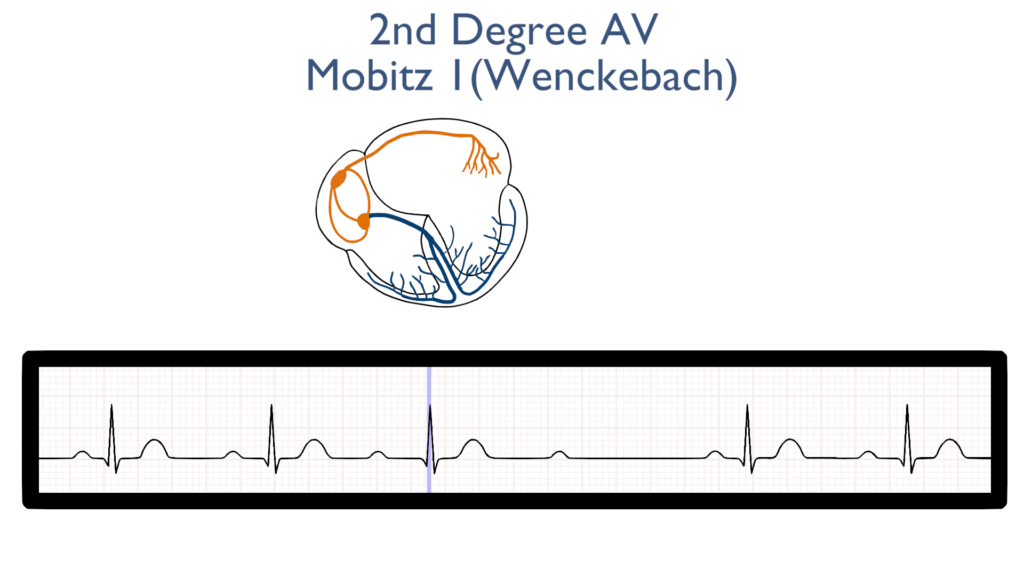
Ventricular Contraction
Next, the impulse travels through the bundle of HIS to the bundle branches and on to the purkinje fibers causing ventricular contraction.
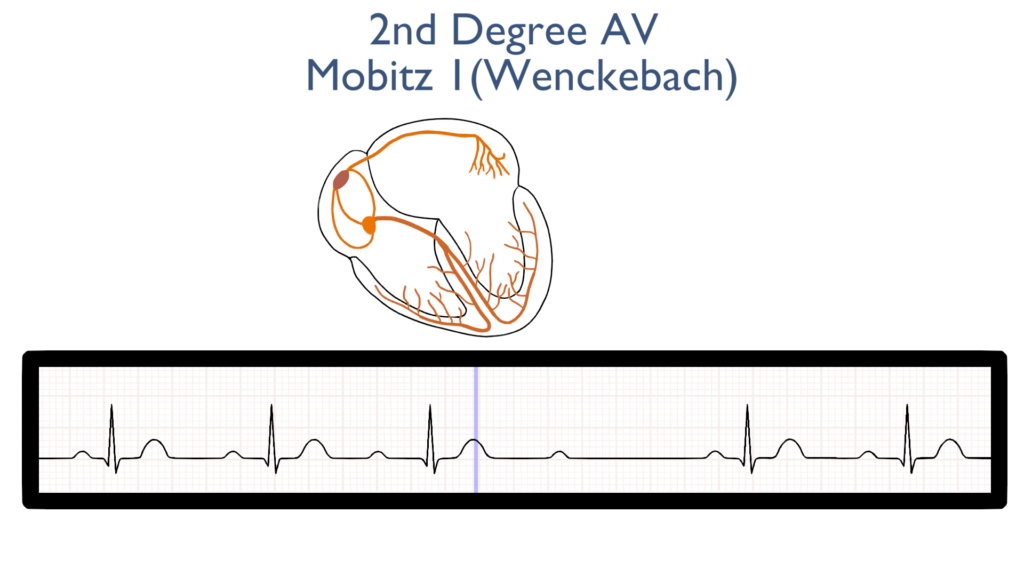
Ventricular Repolarization
Lastly, the ventricles relax and reset for the next contraction.
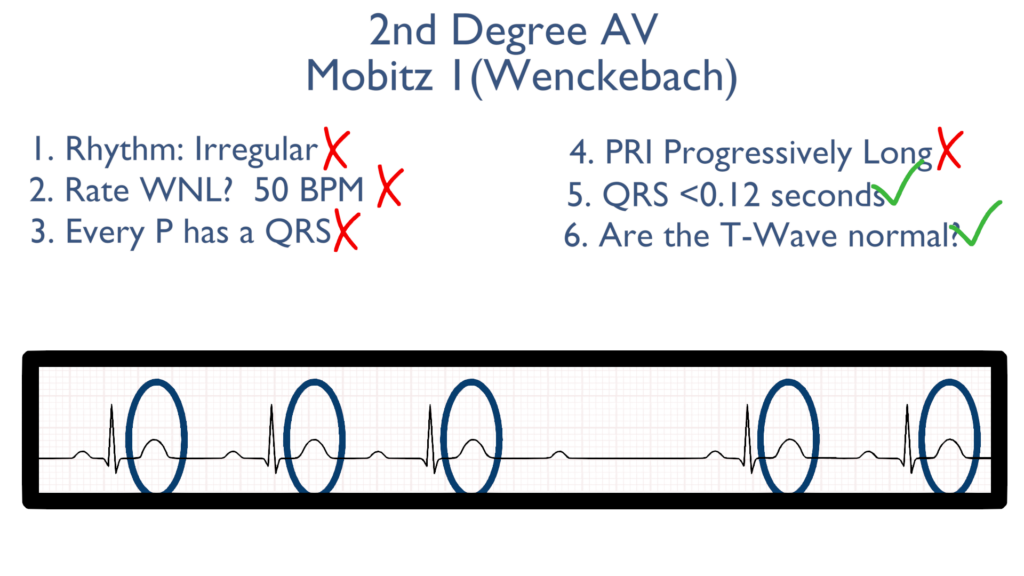
T waves should be normal.
Seven steps of rhythm interpretation
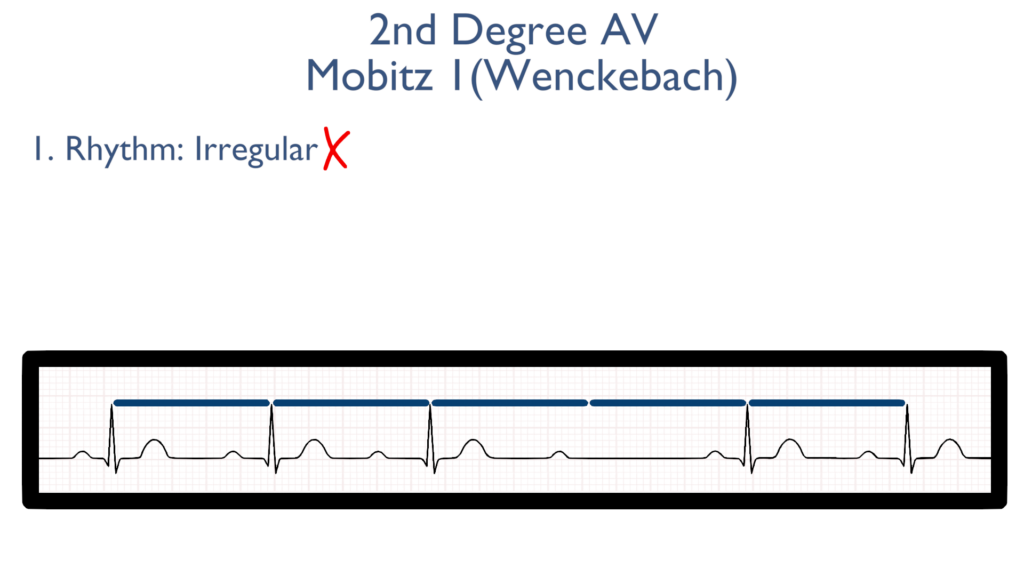
1. Assess the rhythm.
First, the rhythm may be regular or just slightly irregular.
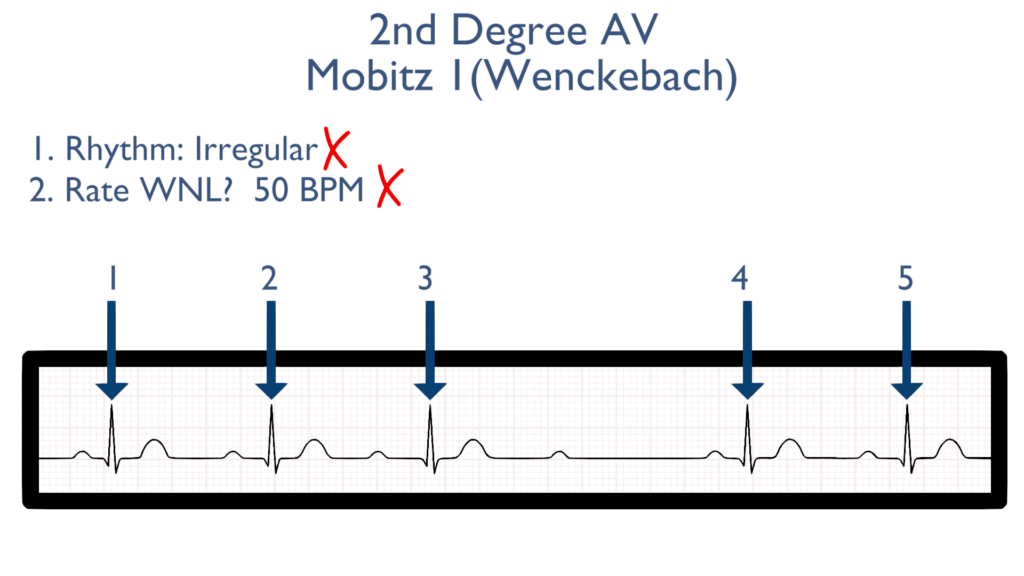
2. Assess the rate.
Next, when assessing the rate you will find it will be variable like the rhythm. The rate may be regular or brady.
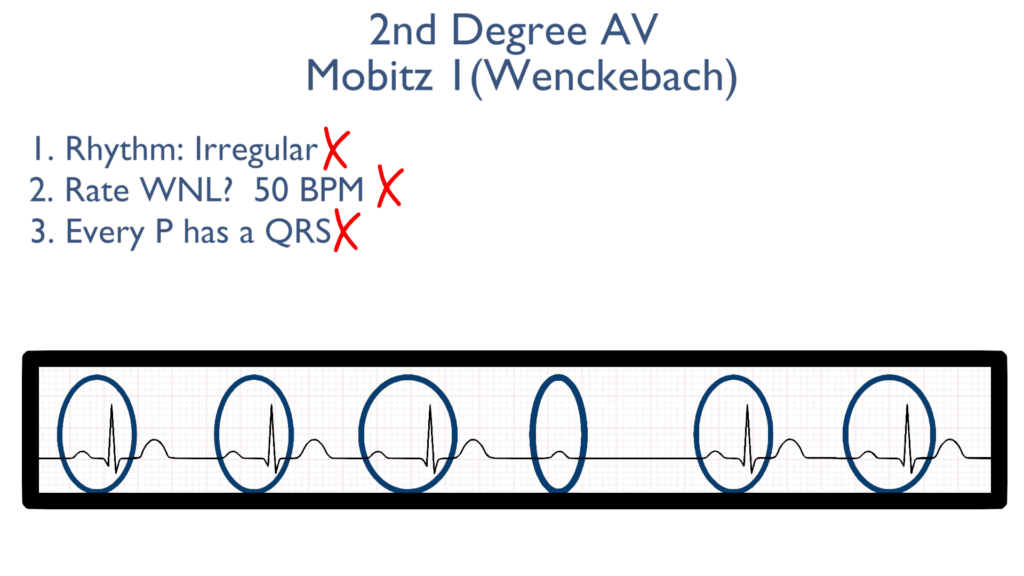
3. Assess atrial and ventricular rates.
When it comes to assessing atrial and ventricular rates there will be more P’s than there are QRS waves.
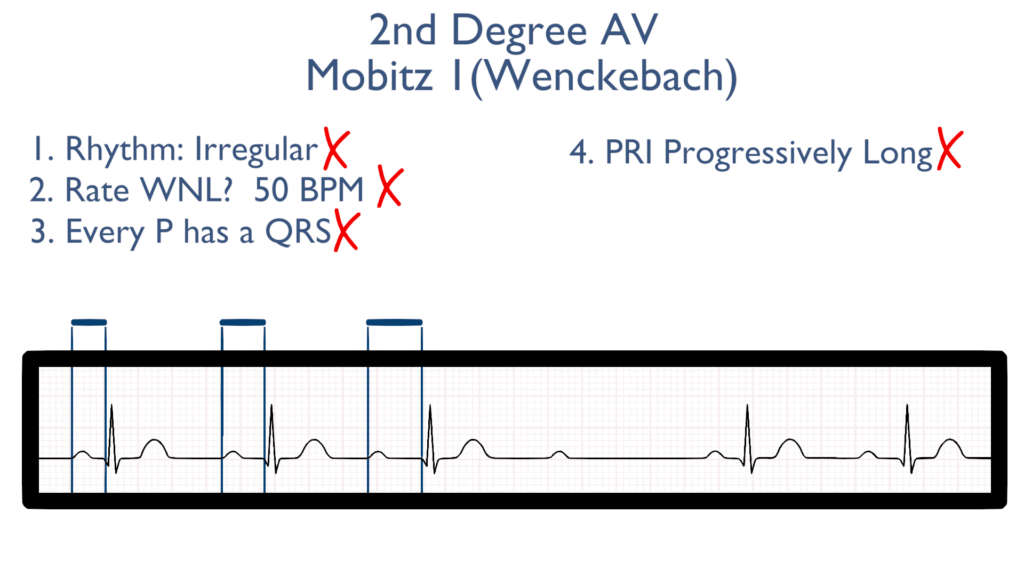
4. Assess the P waves and PR interval.
While the P waves may look normal the PRI will be variable. The PRI will progressively get longer until there is a dropped impulse through the AV node.
After the missed QRS the next PRI will “reset” and be back to it’s original length in the progression.
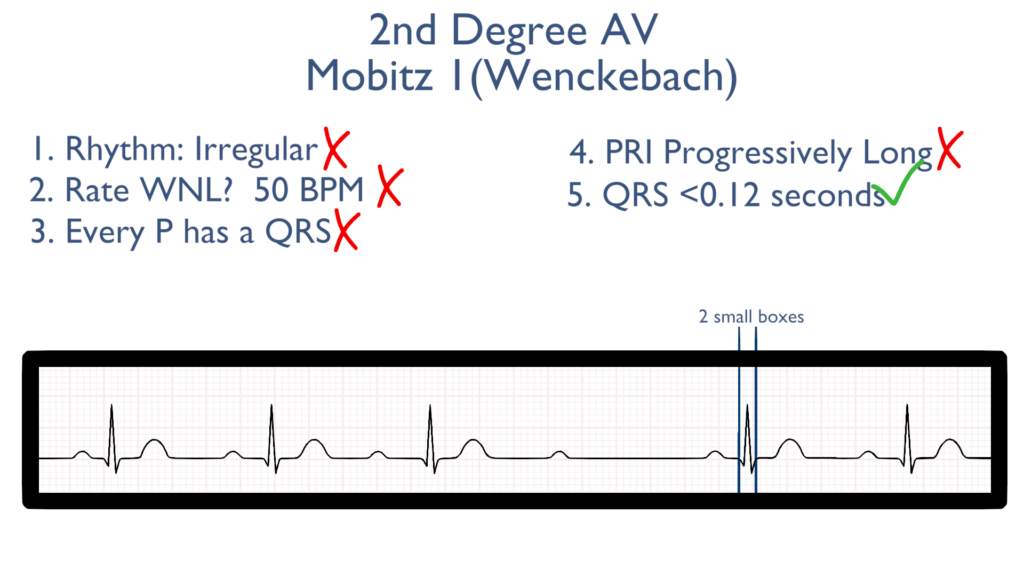
5. Assess the QRS.
Next the QRS will be within normal limits.
The QRS should be between 0.06 seconds to 0.12 seconds.
Better yet, QRS should be between 1.5 to 3 small boxes.
6. Assess the T waves.
T waves should deflect in the positive direction with no ST-Elevation or ST-Depression.
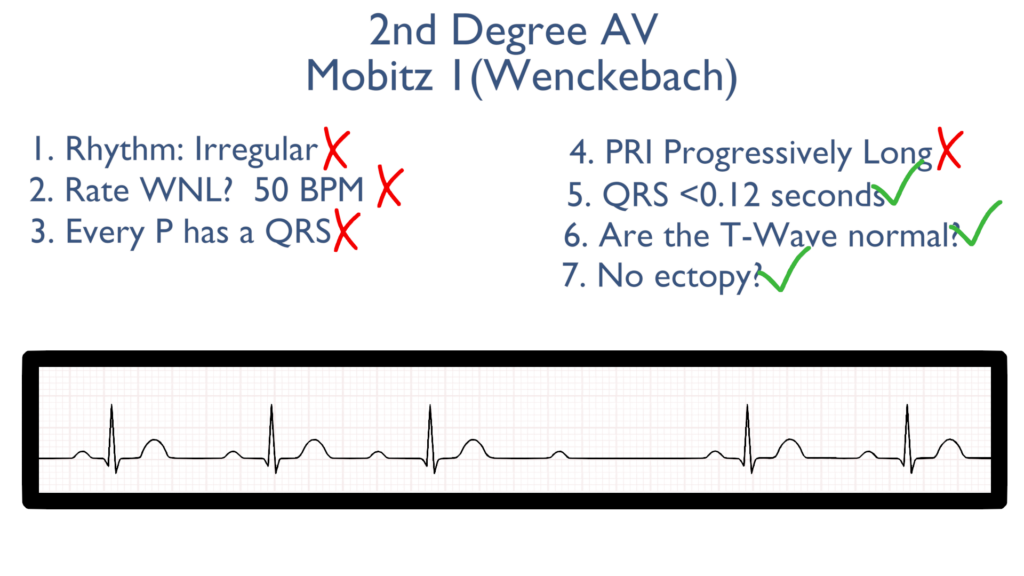
7. Assess for Ectopy.
As you can see on this 6 second strip there are no ectopic beats. This is to say there are no PVC’s or PAC’s present.
Treatments for Mobitz 1 Wenckebach
Stable
i.e. asymptomatic and normotensive
Unstable
i.e. hypotensive with or without symptoms
Pacing (transcutaneous or transvenous) may be considered for treatment.
Medications:
Atropine. (Note: Atropine may be ineffective in Type 2 AV blocks)
Medication Consideration
If this block is caused by medications dosages should be adjusted.