Video
Below is a quick video snap shot of this article.
Definition
When there is no conduction through the AV node which leads to the atria and ventricles working independently.
With other AV blocks we saw that there were times when conduction would not pass through the AV node, but for the most part conduction would make it through on with the majority of impulses. With a 3rd degree conduction never makes it through the AV node which then causes the ventricles to create an impulse on their own.
Consider the fact that the the atria and ventricles are working independent of each other as you read on through this article.
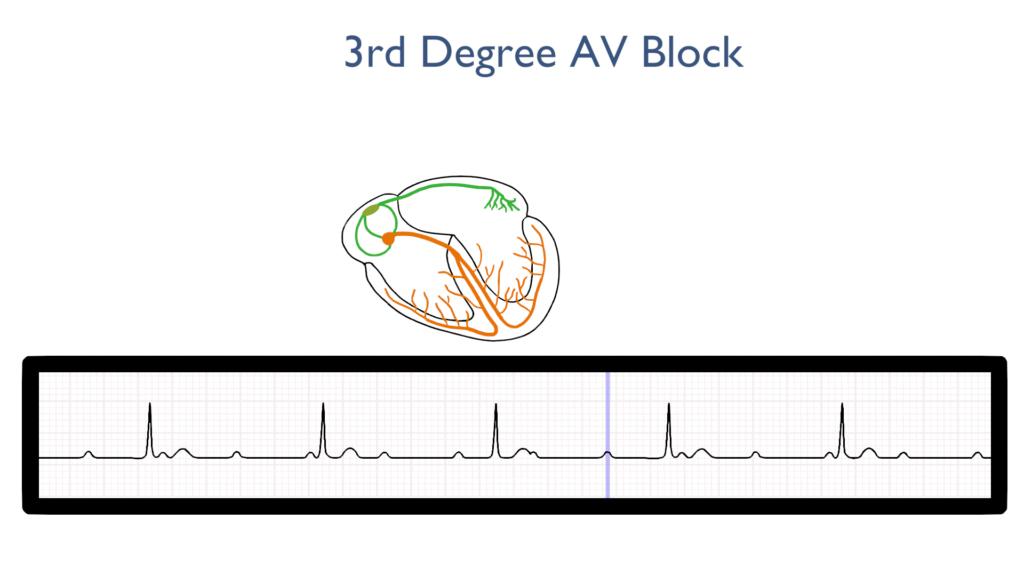
What’s happening in the heart
Atrial Contraction
With atrial contraction the impulse originates within the SA node just as it does with a NSR.
As the impulse approaches the AV node it fails to enter the AV node causing a loss of impulse down to the ventricles.
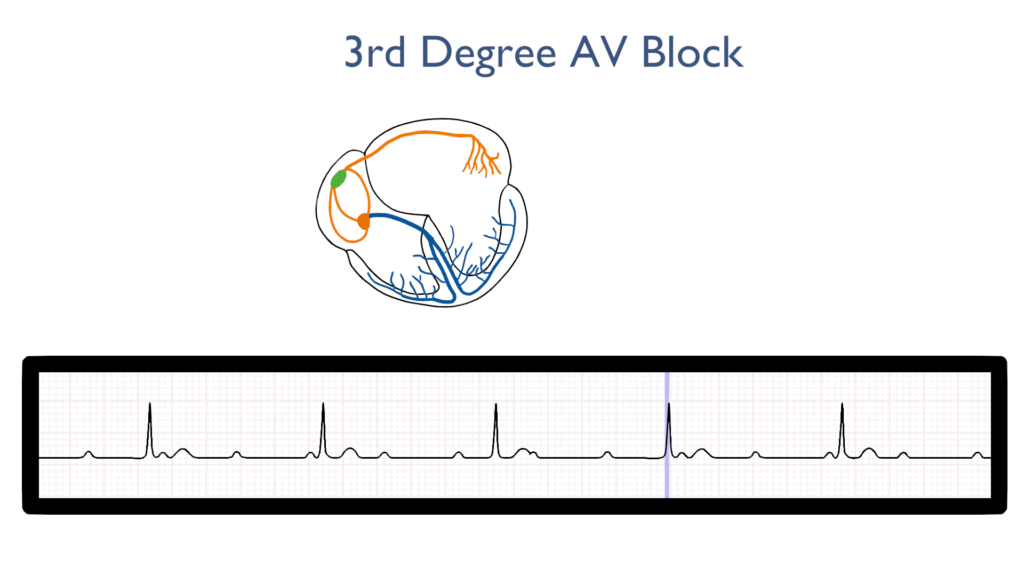
Ventricular Contraction
With ventricular contraction a different impulse originates at or below the AV node causing ventricular contraction.
Some QRS complexes may take the form of PVC’s depending upon how far from the AV node they originate.
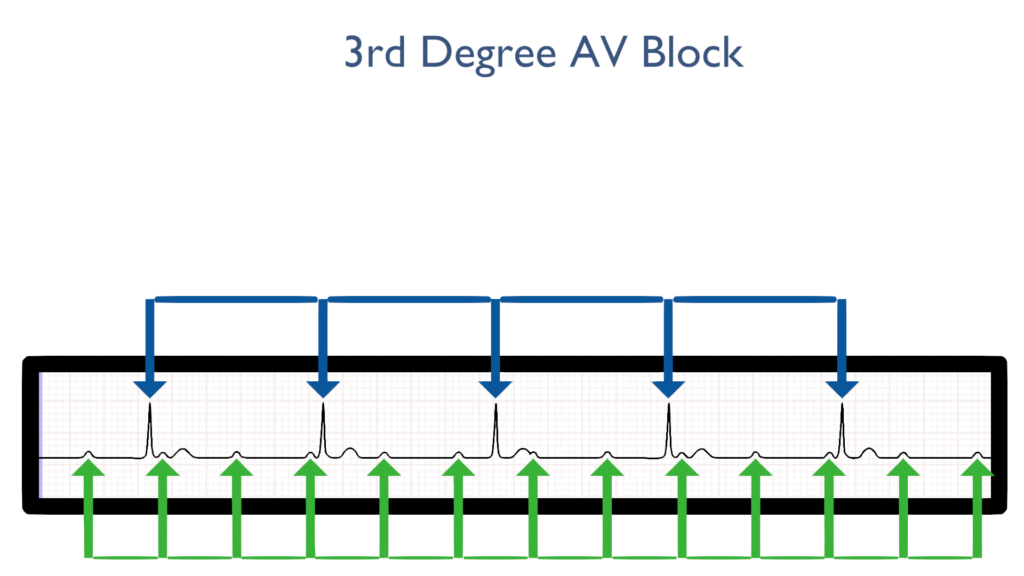
Rhythm Explanation
There are two things to note here:
First, as you can see the rhythm is awkwardly regular. That is to say the ventricular rhythm is regular and the atrial rhythm is regular, but their regularity does not match one another.
Second, while the rhythm is regular with respect to either the atria or ventricle, the rates follow suit. Atrial rates will be within normal limits or above while ventricle rates will be below normal limits.
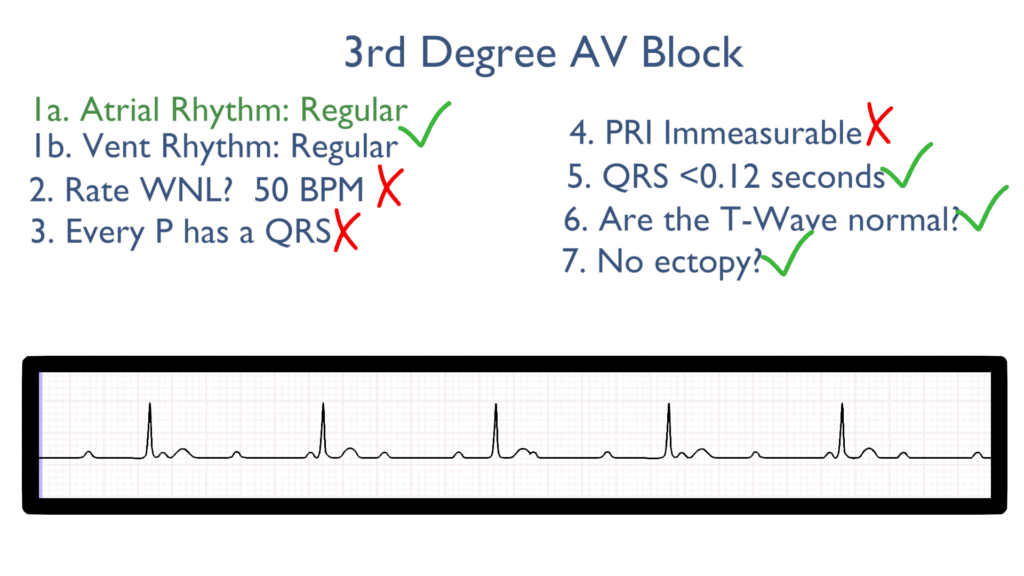
Seven steps of rhythm interpretation
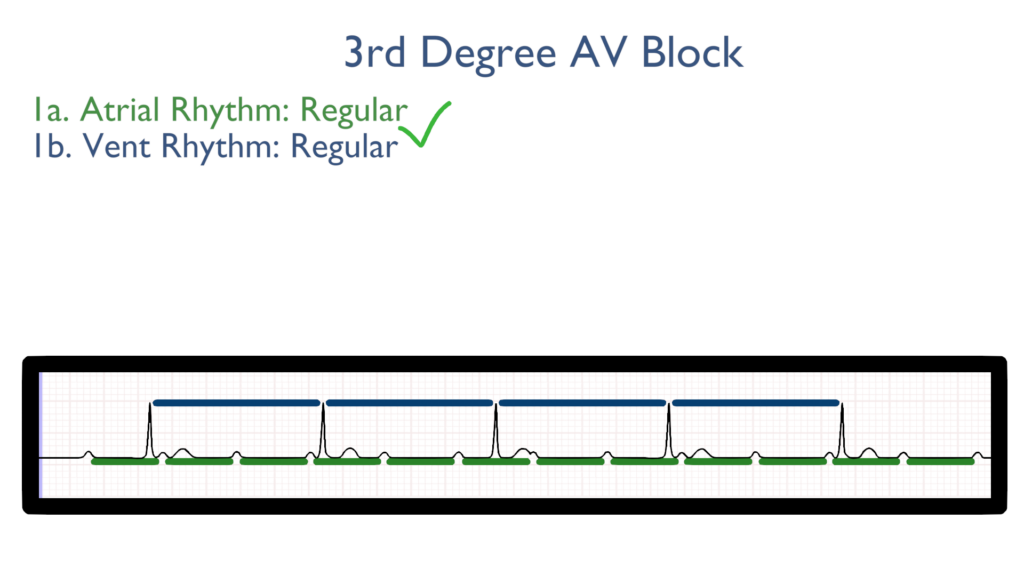
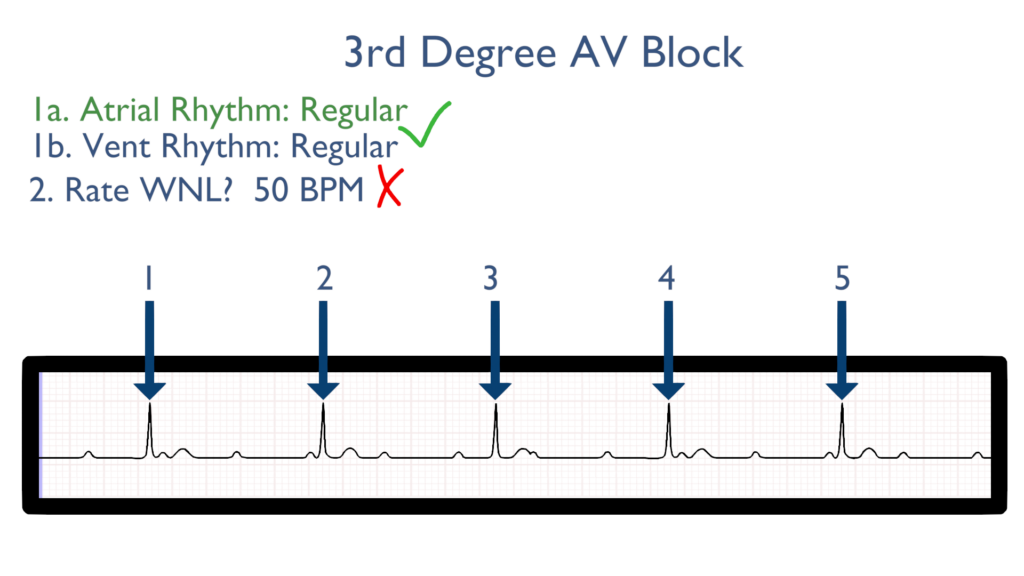
1. Assess the rhythm.
First, as mentioned above, the rhythm will be regular with respect to either the atria or ventricle but the atria and ventricle rhythms will not match up.
2. Assess the rate.
Next, when assessing the rate you will find that the ventricular rate will be less than 60.
When assessing the atrial rate you will notice that the atria will be contracting greater than 60 times a minutes, or better said the atrial rate will be greater than 60.
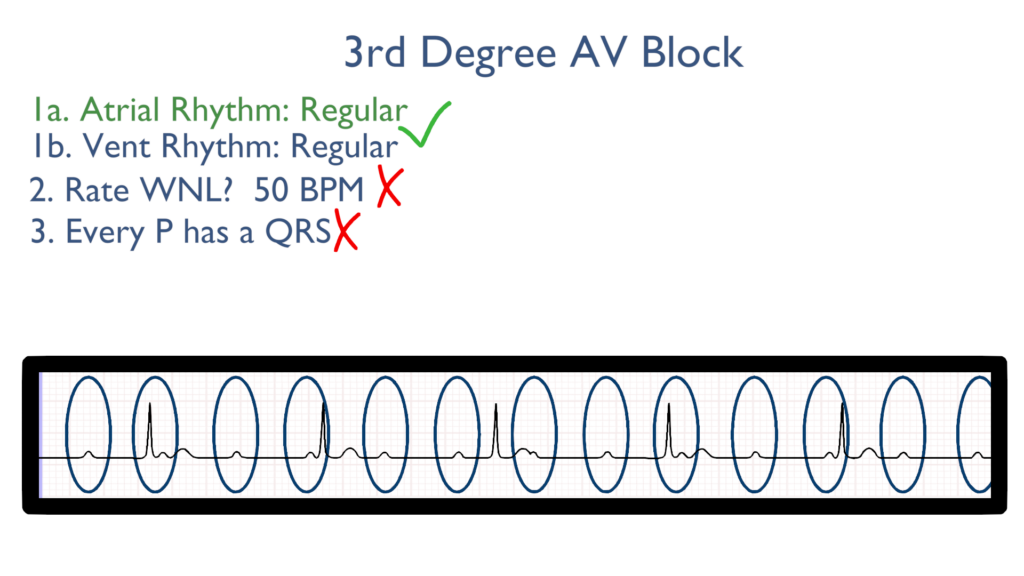
3. Assess atrial and ventricular rates.
As mentioned above, with a 3rd degree you will have a greater amount of P’s than there are QRS.
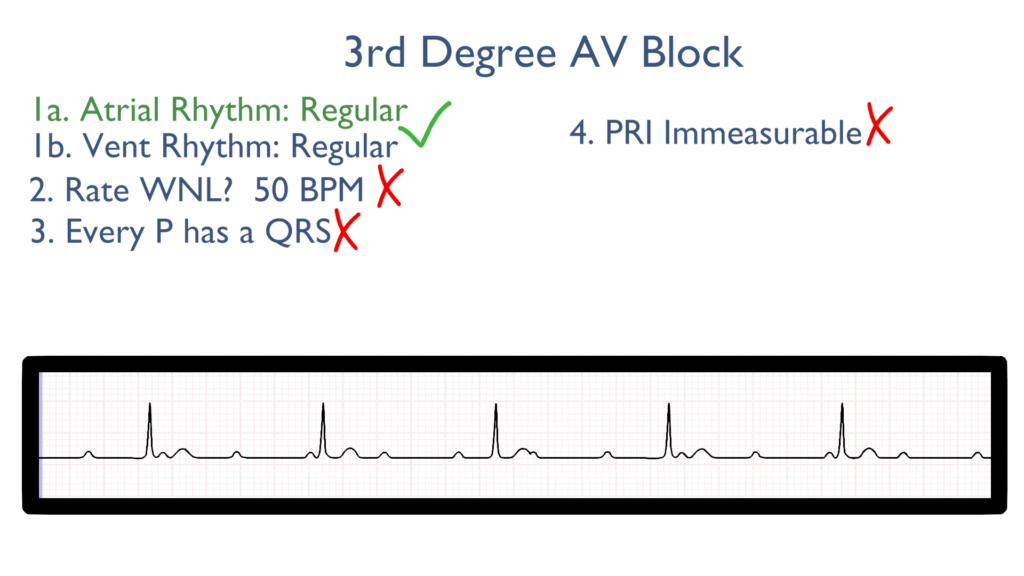
4. Assess the P waves and PR interval.
The PRI will be immeasurable due to the fact that the atria and ventricles are not working together as they should be.
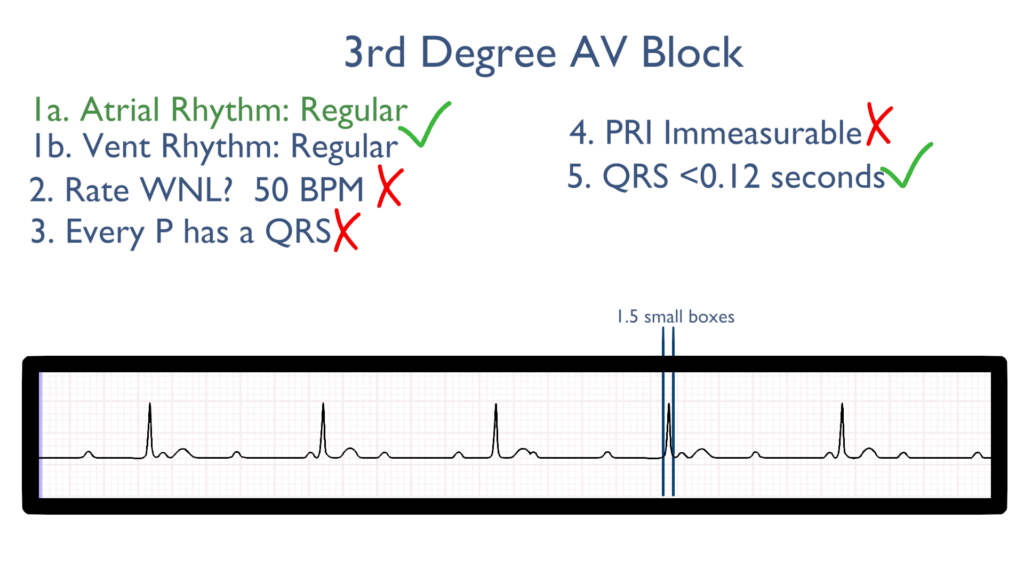
5. Assess the QRS.
With a 3rd degree the QRS will be within normal limits.
6. Assess the T waves.
As with the QRS the T waves should be normal.
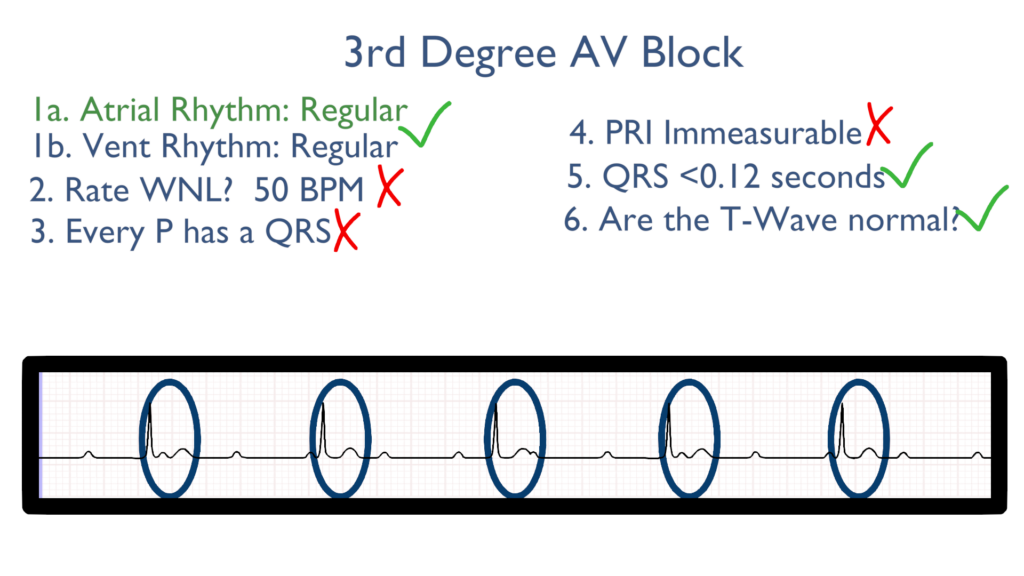
7. Assess for Ectopy.
As you can see here there are not PVC’s or PAC’s.
While the QRS waves make take the appearance of a PVC they do not count as PVCs.
To identify if a PVC happened you should measure the R to R interval. If there is an irregular R to R interval then you may count that QRS as a PVC.
Remember the ventricular rhythm should be regular!
Treatments for
Stable
i.e. asymptomatic and normotensive
Stable patients will eventually need pacemaker placement.
Unstable
i.e. hypotensive with or without symptoms
Pacing (transcutaneous or transvenous) with an end goal of permanent pacemaker placement.
Epinephrine
Dopamine
Medications may be unsuccessful in treating a 3rd degree.
While some medications may bring temporary relief unstable patients will need cardiac pacing.
Note: For most brady rhythms atropine is a preferred medication. With a 3rd degree atropine will not be successful because it acts directly on the SA node. Remember that with a 3rd degree the impulse from the SA node fails to conduct throughout the entire heart, so atropine may have effect on atrial contraction but will have no effect on the ventricular contraction due to the ventricles generating their own impulse.